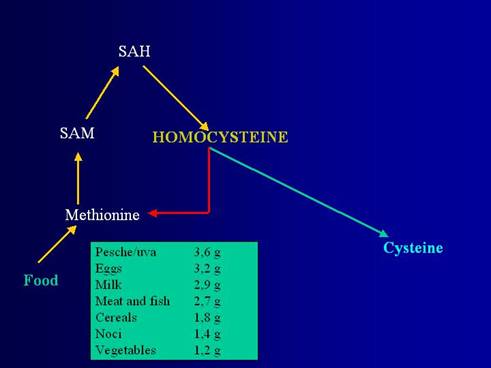
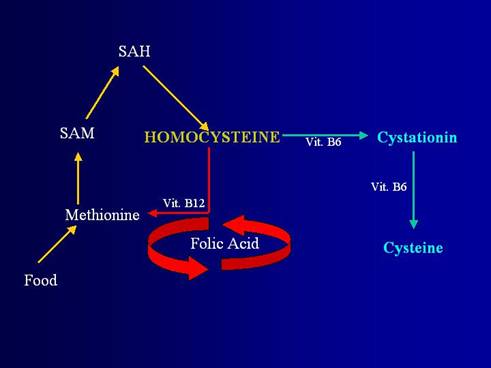
Homocysteine is an intermediary amino acid in the pathway of methionine metabolism.
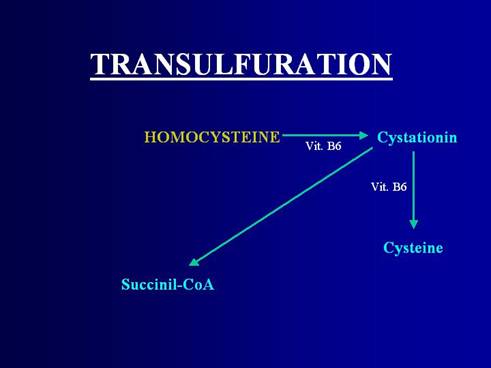
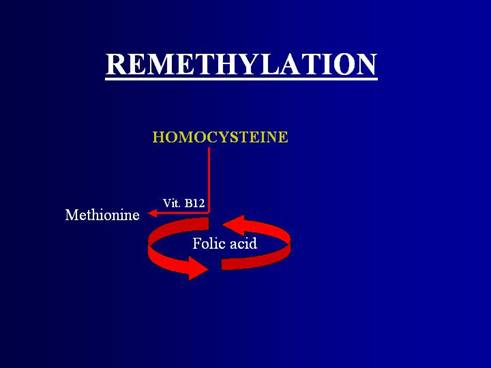
Intracellular homocysteine Is metabolised by either transulfuration or remethylation to methionine.
The metabolism of homocysteine requires intervention of folic acid, pyridoxine and cobalamin.
Elevated plasma homocysteine concentrations are considered an independent risk factor of coronary artery disease and predictor of mortality risk.
It is unclear if homocysteine can be reduced by diet and/or vitamin therapy.
We have studied the hypothesis that supplementation with concentrated fruit and vegetables decreases tHcy levels.
Thirty healthy men and women (15 men and 15 women), aged 20-56 yrs were recruited.
The study was conducted in Foggia, a city of southern Italy.
Exclusion criteria were: pregnancy, breast-feeding, gastrointestinal disorders, use of vitamins and/or minerals, vegetarianism restricted caloric diets, regular intake of medicine, yeast or seaweed, malaria prophylactics or anti-convulsants in the 4 months prior to the study.
On the basis of these criteria, 26 subjects (12 men and 14 women) were considered eligible for participation in the trial. Written consent was requested from all participants for enrolment in the study.
The subjects under treatment took the fruit and vegetables concentrate twice a day for 4 weeks. No alimentary restrictions or changes in life-style were requested.
Product. For the test, a product that is presently on the market and made up of fruit and vegetable powder was used.
Supplementation: 2 capsules of fruit in the morning and 2 vegetables in the evening.
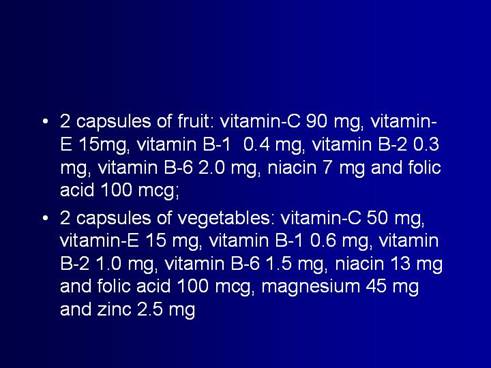
capsules of fruit contain 1.7 grams of concentrated, powdered fruit extract (from apples, oranges, pineapples, blueberries, peaches and papaya)
capsules of vegetable contain 1.7 grams of concentrated, powdered vegetable extract (from carrots, parsley, beet-root, broccoli, black cauliflower, cabbage, spinach and tomato)
This is the dosages of vitamin and minerals present in the capsules.
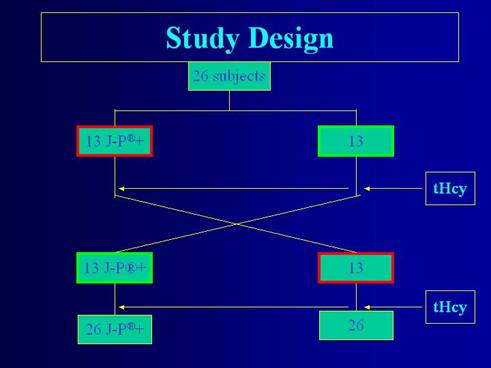
Design. The study was conducted according to a case-cross-over study design, with subjects assigned at random to the treatment group and to the control group (fig. 1). The cross-over, using subjects as their own controls enabled control of the possible confounding factors such as sex, age, dietetic habits and smoking.
The trial was divided into three time periods, each one consisting of 28 days: the first treatment period, wash-out and the second treatment period. During the 1st 27-day treatment period (days 0 to 27) the 13 subjects assigned to Group 1 were supplemented daily with 2 capsules each of the powdered fruit and vegetable extract in the morning and evening, respectively, while the 13 subjects of Group 2 received nothing. Following treatment period 1, both groups were subjected to a 28-day wash-out period (days 28 to 55). During the 2nd 27-day treatment period (days 56 to 82), Group 2 received capsules of fruit and vegetable extract daily while Group 1 received nothing.
One plasma sample was collected of each participant on these days in order to detect tHcy concentrations; another sample collected for determine serum folic acid levels: on day 0 and on day 27 for group 1; on day 56 and on day 83 for group 2.
Dietary intake was estimated by means of food diary in which participants kept a record of their daily food intake throughout the study period.
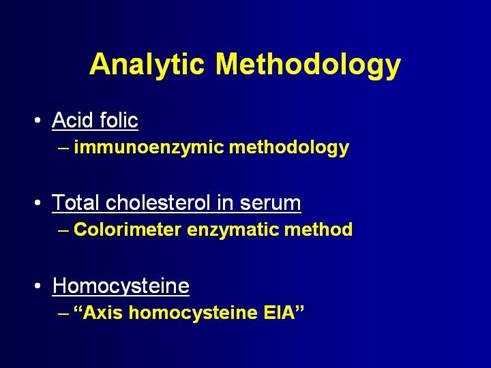
In this picture we report the Analytical Methodology.
The characteristics of the participating subjects are shown in table . 12 men and 14 women with an average age of 35.6 years and a body mass of 24.2 participated.
10 subjects regularly performed physical activities, 3 were smokers. The average level of cholesterolemia was at 155.7 mg/dL.
Most of the subjects normally consumed 1-2 portions of fruit and vegetables a day.
The tHcy levels in plasma decreased throughout each period of treatment but not during the control periods of the study.
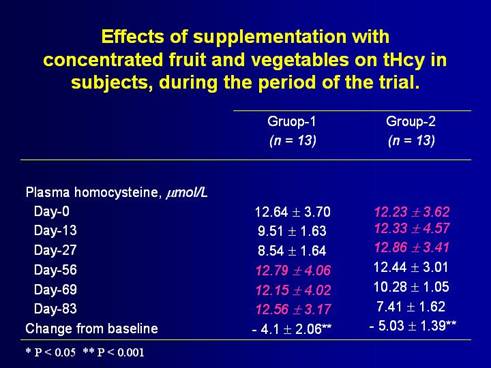
In table the results relative to supplementation and its effect on tHcy in the subjects during the period of the trial are shown.
tHcy levels decreased significantly in both groups.
In group 1 the decreased was 4.1 umol/L from day 0 (starting day of consumption of product) to day 27 (end of treatment);
for group 2, tHcy decreased by 5.03 (± 1.39) from day 56 (beginning of consumption) to day 83 (end of treatment), whereas plasma tHcy changed little during control periods for both groups.
If you pay attention, you cane see how the homocysteine goes up in group 1 in the control period. For us this is unexpected result.
I want underline a phenomenon that we didn’t await. In group one, the tHcy came up in the second period of trial at the same level of starting day.
In this table the results of plasma tHcy levels are shown for subjects during both of the case cross-over periods of the study. During treatment periods when subjects took the powdered extract plasma tHcy steadily decreased, by 2.34 (± 2.82) umol/L half-way through and by 4.73 (± 1.53) umol/L by the 27th day of supplementation compared to controls.
This controlled dietary intervention study demonstrated that the daily consumption of 2 capsules of concentrated fruit and 2 capsules of concentrated vegetables has significantly decreased plasma tHcy levels in 26 subjects whose normal fruit and vegetable consumption is low. THcy levels decreased from an average of 12.71 (±3.23) during the control period to 7.98 (±1.70) during the treatment period. Subjects, were asked not to change their lifestyle, and each participant acted as his/her own control.
In conclusion, we have shown that daily intake of supplements of powdered fruit and vegetables extracts in capsular form significantly decreased plasma levels of tHcy in healthy subjects, just as the interruption of intake allowed tHcy return to pre-supplementation levels. A homocysteine lowering effect may be only part of the health benefit associated with consuming fruit and vegetable extracts on a daily basis. In the other study, the same product decreased DNA damage in the peripheral lymphocytes of an elderly population.
Further studies are in course to demonstrate if the decrease of tHcy is associated with a decrease of the risk of pathologies in which it is implicated. However, already the results of the first studies are encouraging. For example, in a prospective study of 4.4 years, Peterson et al. found that after Hcy-lowering treatment with vitamin supplementation, the rate of progression of carotid plaque formation before and after supplementation was significantly reduced [28]. If this were to be confirmed by other research it would mark a decisive move forwards in the nutritional prevention of disease.
Homocysteine is an epiphenomenona of micronutrients deficiency. We suppose that these deficiencies are new challenge for Medicine. All we are running the risk of suffer the consequences of micronutrients deficiency. Because there is a growing gap of caloric requirement, on one hand, and micronutrients request on the other hand. The caloric requirement reduces why our society is more and more sedentary, through force of use of technology in ours lives. While, micronutrients request is that of mankind and ranges into small intervals.
In practice, we need to eat food with low calories and with right concentrations of micronutrients. Unluckily, several studies shown that synthetic vitamins don’t work very well. On the contrary, they could have negative effects for health.
This is new frontier of nutrition and it puts new questions for us. I think that we need a new paradigm to deal with micronutrient deficiencies under point of view of prevention and therapy of diseases.
A new paradigm that doesn’t bridle us in reductionism of Medicine. We must see that we don’t make the same mistakes of the baby elephant of Deepak Chopra.
Thank you very much.